By A. Hauke. Ashland University. 2018.
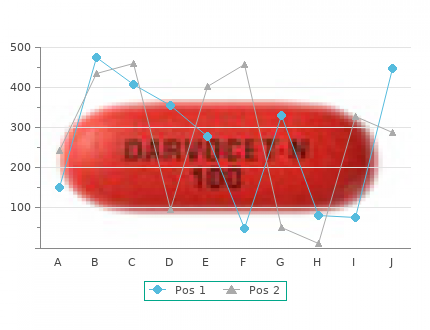
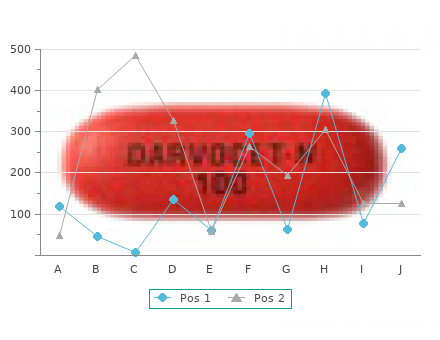
Clinical rating scales are extremely useful kamagra polo 100mg discount, but ratings may be investigator dependent and are frequently confounded by changes in symptomatic treatment buy generic kamagra polo 100mg line. Pathological studies investigating rate of progression have been limited and rely entirely on cross-sectional data (62 buy kamagra polo 100mg mastercard,63) discount 100 mg kamagra polo otc. These studies have in general considered patients with severe illness of long duration. In vivo imaging studies provide the opportunity to evaluate patients longitudinally from early to late disease using an objective biomarker for dopaminergic degeneration. In several studies neuroreceptor imaging of the nigrostriatal dopami- nergic system has been used as a research tool to monitor progressive dopaminergic neuron loss in PD. In longitudinal studies of PD progression 18 both F-DOPA and DAT imaging [b-CIT(2b-carboxymethoxy-3b(4- iodophenyl)tropane) and CFT] using both PET and SPECT have 18 18 demonstrated an annualized rate of reduction in striatal F-DOPA, F- 123 CFT, or [ I]b-CIT uptake of about 6–13% in PD patients compared with 0–2. Similar findings have been reported for VMAT2 imaging (K. Evidence from studies of hemi-PD subjects provide further insight into the rate of progression of disease. In early hemi-PD there is a reduction in 18 F-DOPA and DAT uptake of about 50% in the affected putamen and of 25–30% in the unaffected putamen. Since most patients will progress clinically from unilateral to bilateral in 3–6 years, it is therefore likely that the loss of these in vivo imaging markers of dopaminergic degeneration in the previously unaffected putamen will progress at about 5–10% per annum (11,65). Imaging has also been used to monitor progression of PD in patients receiving fetal substantia nigral transplants for PD. Several studies during 18 the past several years show an increase in F-DOPA uptake with follow-up 18 of 6 months to 6 years posttransplant (90,91). The change in F-DOPA Copyright 2003 by Marcel Dekker, Inc. Note the 123 asymmetric reduction in [ I]b-CIT uptake more marked in the putamen than caudate in the patient and the progressive loss of activity. Levels of SPECTactivity are color-encoded from low (black) to high (yellow/white). The most important role of longitudinal imaging studies is to provide a tool to assess objectively potential neuroprotective and restorative therapies for PD. Imaging studies assessing progression of disease have provided data to estimate sample sizes required to detect slowing of disease progression due to study drug treatment. The sample size required depends on the effect of the disease-modifying drug and the duration of exposure to the drug. The effect of the drug is generally expressed as the percent reduction in rate of loss of the imaging marker in the group treated with the study drug versus a control group. More specifically, imaging studies have 18 sought a reduction of between 25 and 50% in the rate of loss of F-DOPA 123 or [ I]b-CIT uptake (i. The sample size needed to detect a 25–50% reduction in the rate of loss of F- DOPA or b-CIT uptake during a 24-month interval ranges from approximately 30 to 120 research subjects in each study arm (85,93). These data support the use of dopamine neuroreceptor imaging to assess the effects of potential neuroprotective drugs in PD, but there are several caveats in the study design and interpretation of these studies. It must be acknowledged that imaging outcomes in studies of PD patients are biomarkers for brain activity, but are not true surrogates for drug effects in PD patients (94). These investiga- tional drugs may have effects on dopamine neurons unrelated to slowed neuronal degeneration and may have effects outside the dopaminergic system. The rate of change in imaging outcomes used to measure disease progression is slow, reflecting the slow clinical progression in PD and requiring the duration of these progression studies to be at least 18–24 months. In a recent study evaluating potential disease modifying effects of Neuroimmunophilin A, the study duration of 6 months resulted in an equivocal outcome necessitating a second, longer study to clarify the drug effects (95). Progressive loss in brain dopaminergic imaging activity also occurs in aging healthy individuals, though at a rate approxi- mately one-tenth that of PD patients (13,29). The reliability of the imaging outcomes must be assessed. Recent test-retest studies using current technology and analyses metho- dology show good test-retest reproducibility of approximately 3– 18 5% for F-DOPA or VMAT2 studies and 5–7% for b-CIT SPECT (95–97). Imaging outcomes of disease progression may be confounded by pharmacological effects of the study drug. In preclinical studies evaluation of the effect of dopamine agonists and antagonists and levodopa suggest possible regulation of both the DAT and dopamine turnover (32,98).
The monomeric G protein Ran containing bound GTP binds to one of the subunits of importin kamagra polo 100 mg fast delivery. This causes dissociation of the importin subunits and release of the imported protein in the nucleus buy discount kamagra polo 100mg. On the cytoplasmic side 100 mg kamagra polo for sale, a RanGAP (GTPase activating pro- tein) activates the hydrolysis of GTP to GDP discount kamagra polo 100 mg online, which causes dissociation of the complex. RanGDP is subsequently returned to the nucleus, where an accessory protein activates dis- sociation of GDP and association of GTP. CHAPTER 10 / RELATIONSHIP BETWEEN CELL BIOLOGY AND BIOCHEMISTRY 175 RNAs are transported from the nucleus to the cytoplasm as ribonucleoproteins, which are targeted for export by a specific amino acid sequence called the nuclear export signal. The nucleoprotein forms a complex with additional proteins called exportins and with Ran. This complex is transported through the pore to the cyto- plasm, where RanGAP activates hydrolysis of the bound GTP. In the absence of GTP, the complex dissociates with the release of RNA into the cytoplasm, and the exportins and Ran are transported back to the nucleus. ENDOPLASMIC RETICULUM The endoplasmic reticulum (ER) is a network of membranous tubules within the cell Chronic ingestion of ethanol has consisting of smooth endoplasmic reticulum (SER), which lacks ribosomes, and increased the content of MEOS, the rough endoplasmic reticulum (RER), which is studded with ribosomes (Fig. It contains enzymes for the synthesis of many tem, in Al Martini’s liver. MEOS is a cytochrome P450 enzyme that catalyzes the lipids, such as triacylglycerols and phospholipids. It also contains the cytochrome conversion of ethanol, NADPH and O2 to P450 oxidative enzymes involved in metabolism of drugs and toxic chemicals such acetaldehyde, NADP , and 2 H2O (see Chap- as ethanol and the synthesis of hydrophobic molecules such as steroid hormones. The adjective microsomal is a term Glycogen is stored in regions of liver cells that are rich in SER. Ribosomes attached to is sometimes used for processes occurring the membranes of the RER give them their “rough” appearance. When cells are lysed in the labora- on these ribosomes enter the lumen of the RER, travel to the Golgi complex in vesi- tory, the ER is fragmented into vesicles cles, and are subsequently either secreted from the cell, sequestered within called microsomes, which can be isolated by membrane-enclosed organelles such as lysosomes, or embedded in the plasma centrifugation. Posttranslational modifications of these proteins, such as the initiation actually present in cells. In contrast, proteins encoded by the nucleus and found in the cytosol, peroxisomes, or mitochondria are synthesized on free ribosomes in the cytosol and are seldom mod- ified by the attachment of oligosaccharides. A Smooth endoplasmic reticulum (SER) Ribosomes Rough endoplasmic reticulum (RER) B Fig. GOLGI COMPLEX The Golgi complex is involved in modifying proteins produced in the RER and in sorting and distributing these proteins to the lysosomes, secretory vesicles, or the plasma membrane. It consists of a curved stack of flattened vesicles in the cyto- plasm that is generally divided into three compartments: the cis-Golgi network, which is often convex and faces the nucleus; the medial Golgi stacks; and the trans Golgi network, which often faces the plasma membrane (Fig. Proteins are transported to and from the Golgi in at least three kinds of vesicles: coatomer-coated COP I vesicles, coatomer-coated COP II vesicles, and clathrin- coated vesicles (see Fig. Proteins produced on the RER travel in COP II vesicles to an endoplasmic reticulum-Golgi intermediate compartment (ERGIC), and then to the cis-Golgi network, where they enter the lumen. Here N-linked oligosaccharide chains that were added to proteins in the RER are modified, and O-linked oligosaccharides are added. COP I vesicles recycle material from the Golgi back to the ER and possibly transfer material from the Golgi to other sites. Clathrin Trans-Golgi Medial-Golgi COPI Cis-Golgi COPI COPII ER-golgi Fusion intermediate of COPII compartment vesicles Rough ER Fig. COP II vesicles (coatomer- coated) form in the rough ER and move to the Golgi. COP I vesicles generally go from the trans to the cis Golgi to the ER. Vesicles that go to late endosomes (eventually lysosomes) from the Golgi or the plasma membrane are clathrin-coated. Vesicle transport, as well as transport of organelles and secretory proteins, occurs along microtubules (structures formed from the protein tubulin). CHAPTER 10 / RELATIONSHIP BETWEEN CELL BIOLOGY AND BIOCHEMISTRY 177 Vesicles released from the trans face of the Golgi complex travel to endosomes as clathrin-coated vesicles. COP vesicles are coated with a complex composed of coatomer proteins (COP), an Arf family monomeric G protein that mediates vesicle assembly, and other proteins (Fig.
However buy generic kamagra polo 100 mg online, most of these forces are controlled by the ligamentous restraints in the knee joint purchase 100mg kamagra polo free shipping. Hip The hip joint is the only joint with significant motion in all three planes dur- ing gait order kamagra polo 100mg without prescription. The hip is also a principal power output joint along with the ankle 7 cheap kamagra polo 100mg without prescription. Complete control of the knee in- cludes stabilizing function of the hamstrings and quadriceps, especially at foot contact, which is provided by isometric contraction, a hip extensor that uses momentum to ex- tend the hip and knee at the same time. In mid- stance and terminal stance phase, the gastro- csoleus is the primary controller of the knee position. In swing phase, the rectus initially controls knee flexion through an eccentric contraction and the hamstrings use an ec- centric contraction to decelerate the forward swing of the foot, thereby limiting knee ex- tension (A). These motions are well demon- strated on the knee kinematics along with the normal moments and power absorption at the knee. Significantly more power is absorbed at the knee than is generated, demonstrating the fact that the knee’s primary function is to provide stability and change the limb’s length between stance and swing phase (B). The position of hip flexion at initial contact significantly contributes to step length along with knee extension. At initial contact, the hip starts into extension under the influence of strong gluteus maximus con- traction. Additionally, all of the hamstring muscles plus the adductors are active at initial contact and remain active during weight acceptance phase. This forceful hip extension provides a large hip extension moment in early stance phase and a power output to lift the forward falling of the body. Also, at initial contact and in weight acceptance, the abductor muscles are active to contract and hold the center of gravity in the midline. There is an initial hip adduction motion in weight acceptance followed in midstance and terminal stance with gradual abduction. In mid- and terminal stance, the hip abduc- tors and extensor muscles are relatively quiet, with the fascia latae being con- sistently active. Middle stance is a time of low-level muscle activation as mo- mentum provides primary stability with only minimal control by the fascia latae. During terminal stance and preswing, the adductor muscles become active and act as hip flexors and adductors. In terminal stance, the hip flex- ion is again initiated, which can occur passively as an effect of the momentum of the body moving forward off the planted foot and the forceful contraction of the ankle plantar flexors. This force provides transfer of momentum from knee flexion into hip flexion by the rectus as the rectus activates to decrease the acceleration and control the magnitude of knee flexion (Figure 7. The other alternative is a concentric contraction of the primary hip flexors, which include the iliacus and psoas muscles. Also, the secondary hip flexors, in- cluding the gracilis, adductor longus, and brevis, may be active. During swing phase, there is gradual hip adduction correlated with hip flexion. In general, the hip flexors adduct and internally rotate and the pri- mary extensor muscles abduct and externally rotate the hip (Figure 7. Early stance phase is a major time of power generation at the hip, second only to the late stance push-off power burst of the gastrocsoleus at the ankle to provide the force, which propels the body forward. This power is primarily generated from the gluteus maximus extending the hip as momentum is driving the forward-falling body. During midstance, there is little power absorption or generation; however, in terminal stance and preswing, the power burst occurs secondary to the active force output to generate forward motion of the leg through hip flexion. In middle swing, there is very little muscle activity; however, by terminal swing, the hip ex- tensors, especially the hamstrings and gluteal muscles, are again becoming active to decelerate the forward swing of the shank and foot, and transfer that force into hip extension. Pelvis The pelvis moves through space in a motion akin to swimming, with a com- bination of pelvic anterior and posterior tilt, pelvic obliquity, and pelvic ro- tation (Figure 7.
If the osteotomy is made too close to the insertion of the blade plate kamagra polo 100 mg lowest price, there may be a fracture of the lateral bridge of the proximal fragment (Case 10 buy kamagra polo 100 mg low cost. This fracture can be avoided by ensuring that there is an adequate lateral bridge or ensuring that the distance from the insertion of the blade plate to the osteotomy site is wide enough 100mg kamagra polo overnight delivery. A common error is measuring the hy- potenuse of this triangle instead of its direct right angle leg and thereby getting a lateral bridge that is too narrow cheap kamagra polo 100 mg with visa. The fixation of the blade plate requires a strong lateral cortical buttress against which compression can be applied. If a lateral fracture occurs and there is room in the femur, the blade plate should be moved more proximally and placed into the center of the femoral neck as far as possible into the femoral head. Often, this means that a plate with more added valgus has to be used and a lateral cerclage wire is generally required because there is not enough lateral bone for the compres- sion. It is important for surgeons to remember that the blade plates may be bent into more of a valgus position if the need arises. The problem with put- ting too much valgus into the plates, however, is that the ability to compress the osteotomy site, which is important to prevent nonunions, is lost. This is why these plates are made only in 90° and 100° angles. A radio- seen with in-toeing due to increased anteversion. A de- graph was obtained that showed a proximal femoral frac- rotational proximal femoral osteotomy was performed ture (Figure C10. He did well postoperatively, being mo- radiographs were carefully reviewed and showed an os- bilized to ambulatory weight bearing as tolerated using a teotomy site that was too close to the blade insertion, walker. Ten days after surgery when he was at home, he therefore making the lateral femoral bone support too narrow. The insertion site should be in the area between the two lateral bends in the plate (Figure C10. The frac- ture may then propagate into the femoral head, with a fragment of the femoral head and neck and trochanter elevating, or only the greater trochanter may fracture free of the plate (Case 10. This fracture can be avoided by never inserting the blade into the apophysis of the greater trochanter and by al- ways staying in or below the subchondral bone of the greater trochanteric apophysis. If the fracture goes into the greater trochanter only, and the greater 10. This created a very demanding three-part oped a left hip dysplasia that slowly progressed and was fracture situation that we resolved with a removal of the believed to merit hip reconstruction. Because of signifi- plate, then fixed the distal two fragments with a small an- cant leg lengthening discrepancy, she also had a femoral terior plate (Figure C10. A new plate was bent to shortening osteotomy on the right side. Although she was the intended degree of varus, approximately 120°, and moderately obese, the operative procedure and postoper- was inserted parallel to the femoral neck until it was just ative course went well until the fifth day postoperatively, short of the epiphysis (Figure C10. This was fol- when the physical therapist reported increased pain with lowed by a cancellous screw inserted above the plate movements of getting her from the bed to chair. A phys- chisel so it got good bone hold right up to the epiphysis ical examination demonstrated increased pain and an (Figure C10. A tension band wire was then inserted external rotation deformity of the femur indicating a through the greater trochanter, pulled down, and twisted probable fracture. The radiograph demonstrated a frac- around the screw, and then brought through a small hole ture proximal to the blade (Figure C10. This left the drilled anterior to posterior in the distal fragment (Figure femur with a free femoral head and trochanter (Figure C10. The tension band wire was tight- #2 and #3) still stabilized with the plate. The cause of this ened so it was lateral to the plate.