By D. Grok. Southern Wesleyan University.
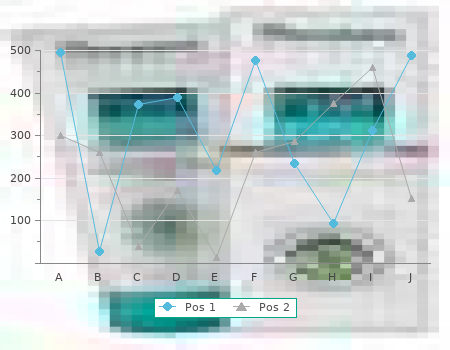
You must indicate from where all the information to which you refer has come purchase 0.1mg clonidine amex, so remember to keep a complete record of everything you read cheap clonidine 0.1 mg with mastercard. If you do not do this cheap clonidine 0.1 mg visa, you could be accused of plagiarism which is a form of intellectual theft clonidine 0.1 mg for sale. When you are referring to a par- ticular book or journal article, find out the accepted stan- dard for referencing from your institution (see below). Methodologyand Methods In this section is set out a description of, and justification for, the chosen methodology and research methods. The length and depth of this section will depend upon whether you are a student or employee. If you are an undergrad- uate student you will need to raise some of the methodo- logical and theoretical issues pertinent to your work, but if you are a postgraduate student you will need also to be aware of the epistemological and ontological issues in- volved. If you are an employee you may only need to pro- vide a description of the methods you used for your research, in which case this section can be titled ‘Research 136 / PRACTICAL RESEARCH METHODS Methods’. Remember to include all the practical informa- tion people will need to evaluate your work, for example, how many people took part, how they were chosen, your time scale and data recording and analysis methods. The con- tent of this section will depend on your chosen methodol- ogy and methods. If you have conducted a large quantitative survey, this section may contain tables, graphs, pie charts and associated statistics. If you have conducted a qualitative piece of research this section may be descriptive prose containing lengthy quotations. Conclusion In this section you sum up your findings and draw conclu- sions from them, perhaps in relation to other research or literature. How- ever, if you are an employee who has conducted a piece of research for your company, this section could be the most important part of the report. It is for this reason that some written reports contain the recommendation section at the beginning of the report. In this section is set out a list of clear recommendations which have been developed from your research. Further Research It is useful in both academic reports and work-related re- ports to include a section which shows how the research can be continued. Perhaps some results are inconclusive, HOW TO REPORT YOUR FINDINGS/ 137 or perhaps the research has thrown up many more research questions which need to be addressed. It is useful to include this section because it shows that you are aware of the wider picture and that you are not trying to cover up something which you feel may be lacking from your own work. This includes all the literature to which you have referred in your report. A popular method is the Har- vard system which lists the authors’ surnames alphabeti- cally, followed by their initials, date of publication, title of book in italics, place of publication and publisher. If the reference is a journal article, the title of the article appears in inverted commas and the name of the journal appears in italics, followed by the volume number and pages of the article. Figure 5 pro- vides a section of a bibliography from a PhD thesis to il- lustrate this method. Bibliography Larger dissertations or theses will require both a reference section and a bibliography. As discussed above, the refer- ence section will include all those publications to which you have referred to in your report. If, however, you have read other work in relation to your research but not actu- ally referred to them when writing up your report, you might wish to include them in a bibliography. However, make sure they are still relevant to your work – including books to make your bibliography look longer and more impressive is a tactic which won’t impress examiners. Example list of references Appendices If you have constructed a questionnaire for your research, or produced an interview schedule or a code of ethics, it may be useful to include them in your report as an appen- HOW TO REPORT YOUR FINDINGS/ 139 dix.
These publications clarified the confusions about association and causation 0.1mg clonidine with amex, relative and absolute risk which discount 0.1 mg clonidine mastercard, as we have seen buy discount clonidine 0.1 mg, have played a major role in the rise of health promotion in relation to diet and CHD purchase clonidine 0.1 mg with amex, passive smoking, and other controversies about risk factors and individual behaviour. They also exposed other examples of statistical scams and tendentious arguments used to justify interventions in lifestyle and screening programmes in relation to a wide range of diseases. The radical statisticians of the left identified so closely with the new public health movement that they were incapable of challenging the specious statistics on which much of the movement’s policies were based. Though the conservative critics of state health promotion provided a valuable service in challenging its authoritarian character and in exposing its cynical manipulation of epidemiology, their attempts to explain the origin of this policy were unsatisfactory and incoherent. Whereas Skrabanek denounced The Health of the Nation policy as ‘health fascism’, Bruce Charlton considered that it resembled ‘a Soviet-style command economy’. The term ‘health fascism’ became popular in tabloid attacks on health promotion, which often focused on Virginia Bottomley who became something of a hate-figure for the Tory right. But Bottomley and Major seemed unlikely Nazis and the rhetoric of ‘informed choice’, ‘non- judgemental’ counselling and ‘empowerment’ that permeated official health promotion appeared far removed from the language of fascism. More importantly, though considered objectively The Health of the Nation had an authoritarian character, it was not perceived as coercive by the vast majority of people. The instinctive 85 THE POLITICS OF HEALTH PROMOTION distaste for health promotion expressed by right-wing libertarians was understandable, but it also reflected their distance from the subjectivity of the British public. Charlton’s parallel between The Health of the Nation and Stalinist ‘command and control’ bureaucracy, with its plans and targets, had an immediate appeal (though Anderson’s epithet ‘food Leninism’ seemed rather forced) (Anderson 1994). While conservative ideologues have never had difficulty in equating fascism and communism, they had a bigger problem reconciling the notion that the government had adopted a state socialist strategy towards health promotion at the very moment that its wider reforms of the health service were proceeding under the influence of an extreme version of the ideology of the free market, as expounded in Working for Patients (DoH 1989). As Charlton recognised, these appeared to be ‘two distinct, and perhaps irreconcilable, philo-sophies of what the NHS is and what it should be’ (Charlton 1994: 51). Behind The Health of the Nation, he discerned a ‘peculiar alliance between the free marketeering right wing and the revolutionary left wing’ (Charlton 1994:55). Of course, no such alliance took place, not least because, by the early 1990s, both these familiar poles of twentieth-century politics had, for all practical purposes, ceased to exist. This made it quite possible for a pragmatic government to synthesise elements from different political traditions (an approach systematically pursued by New Labour under Tony Blair). Though in its twilight phase the Conservative government undoubtedly adopted some irrational measures (such as, for example, the Poll Tax), there was, as we have seen, a coherent thread running through its policies in the sphere of health. In practice, there was no contradiction between The Health of the Nation and Working for Patients. The common theme of both documents was the promotion of individualism, in personal behaviour and in the provision of healthcare. Ironically there was more scope for this under the state-led health promotion policy than there was under the ‘quasi-markets’ in which competition between ‘purchasers’ and ‘providers’ was supposed to flourish. In these documents, which were both given high-publicity launches, style and symbol were as important as substance. In the Health of the Nation, socialist rhetoric provided a popular packaging for an essentially individualistic policy; in Working for Patients, free market rhetoric gave the impression of a more radical restructuring of the NHS than actually took place. The paradox of the new world order of the early 1990s was that, when the state had been rolled back and socialism crushed, the result was not a society of robust and intrepid entrepreneurs, but one of weak and vulnerable individuals. Instead of a climate of opinion which celebrated individual responsibility and autonomy, what emerged was a culture of complaint and victimhood, which elevated the values of safety over those of risk-taking, femininity over mascu-linity, childhood over adulthood (Furedi 1997). Just as the zest for privatisation turned into the pursuit of new forms of state support for faltering enterprise, so the ‘empowerment’ promised by health promotion led to the further medicalisation of personal life and the creation of new forms of dependency. And just as the level of state expenditure required to sustain private enterprise resisted all attempts at retrenchment, so, far from reducing health service spending, health promotion and the rising demands for reassurance it generated, drove costs further upwards. Perhaps the greatest weakness of the right-wing critique of health promotion was its inability to explain the fact that, far from provoking public hostility to its intrusive and authoritarian measures, these were generally received with remarkable passivity, if not outright enthusiasm. On the one hand they argued that the success of health promotion resulted from the more or less conspiratorial and manipulative activities of its propagandists.
Writing the title You might want to write your title as a question or a statement 0.1mg clonidine for sale. Whichever one you choose it must reflect the content of the dissertation and indicate your approach to the topic order 0.1mg clonidine mastercard. Compare ‘The role of infection control mea sures in reducing the incidence of MRSA’ with ‘A discussion about the lim itations of current infection control measures in reducing the incidence of MRSA’ purchase clonidine 0.1mg overnight delivery. Remember to keep the wording precise by eliminating any redundant words or phrases buy 0.1 mg clonidine visa. The structure of your dissertation Your dissertation is most likely to be analytical in nature. Use it to demon strate your in-depth understanding of the subject matter and your ability to analyse and evaluate the information. The structure of your essay will be based on the keywords used in your title. What do you want to achieve with your work (for example, ‘to explore x’, ‘to evaluate y’ or ‘to analyse z’)? For example: A discussion about the limitations of current infection control measures in reducing the incidence of MRSA. The key words are ‘discussion’, ‘limitations’, ‘current infection control measures’, ‘reducing the incidence’ and ‘MRSA’. The themes are: DISSERTATIONS 197 ° infection control measures ° MRSA (incidence of) ° the relationship between infection control and the incidence of MRSA. The essay will examine the evidence for the effectiveness of infection con trol in reducing MRSA. Breaking the essay down into its component parts in this way will help you organise information into a logical sequence. The use of headings is probably advisable considering the length of a dissertation. For example, a section from the above essay might be headed ‘The incidence of methicillin resistant Staphyloccus aureus’. He or she will be able to sup port your studies and advise on the writing up of your project. References A dissertation is a reflection of the broad and in-depth reading you have undertaken during your enquiry. They will help distinguish your original thoughts and ideas from those of other researchers. The nature of these ref erences will also give an indication of whether the information you have used is current or not and the validity of your source material. Supplying a complete and comprehensive reference list will enable the reader to follow up sources for themselves. There are two main styles of referencing: ° the Harvard style ° the Vancouver style. The Harvard style The Harvard or ‘author–date’ system is well known and widely used within academic institutions. For books, the name of the author and the year of publication are placed in parentheses within the main body of the text, for example: 198 WRITING SKILLS IN PRACTICE Use question stems (Polit and Hungler 1995) to help define your enquiry. However, if there is more than one edition of the book then use the date of the revision or edition you are us ing. Include a reference to figures or tables along with author name and date if you are directly referring to this. Direct quotes or references to specific parts of a text must be accompa nied by the author, date and inclusive page numbers. If your reference is part of the text then no parentheses are used for the names. For example, ‘Barnes (1995) suggests…’ Initials are not provided in the text unless you are quoting two differ ent authors with the same last name. References to works by the same author and published within the same year can be distinguished by adding a suffix letter, for example Argyle 1983a. List single author publications first, before co-authored works where the single author is the first name to appear, for example: Argyle 1983 Argyle and McHenry 1971.
The 45˚ supine oblique view shows the intervertebral foramina and the facets but a better view for the facets is one taken with the patient log rolled 22 order clonidine 0.1 mg otc. Flexion and extension views of the cervical spine may be taken if the patient has no neurological symptoms or signs and initial radiographs are normal but an unstable (ligamentous) injury is nevertheless suspected from the mechanism of injury buy clonidine 0.1 mg low cost, severe pain proven 0.1 mg clonidine, or radiological signs of ligamentous injury buy cheap clonidine 0.1 mg line. To obtain these radiographs, flexion and extension of the whole neck must be performed as far as the patient can tolerate under the supervision of an experienced doctor. If there is any doubt about the integrity of the cervical spine on plain radiographs, CT should be performed. This provides much greater detail of the bony structures and will show the extent of encroachment on the spinal canal by Figure 3. It is particularly clearly the facet dislocation at the C5–6 level, less obvious in the 45˚ useful in assessing the cervicothoracic junction, the upper oblique view (right), which, however, shows a malalignment of the cervical spine and any suspected fracture or misalignment. It allows for a faster examination and also clearer reconstructed images in the sagittal and coronal planes. Many patients with major trauma will require CT of their head, chest or abdomen, and it is often appropriate to scan any suspicious or poorly seen area of their spine at the same time rather than struggle with further plain films. MRI gives information about the spinal cord and soft tissues and will reveal the cause of cord compression, whether from bone, prolapsed discs, ligamentous damage, or intraspinal haematomas. It will also show the extent of cord damage and oedema which is of some prognostic value. Although an acute traumatic disc prolapse may be associated with bony injury, it can also occur with normal radiographs, and in these patients it is vital that an urgent MRI scan is obtained. These scans can also be used to demonstrate spinal instability, particularly in the presence of normal radiographs. MRI has superseded myelography, both in the quality of images obtained and in safety for the patient, allowing decisions to be made without the need for invasive imaging modalities. Its use may be limited by its availability and the difficulty in monitoring the acutely injured patient within the scanner. Pathological changes in the spine—for example, ankylosing spondylitis or rheumatoid arthritis—may predispose to bony damage after relatively minor trauma and in these patients Figure 3. This x ray • Pelvic fractures may be the first to reveal an injury to the thoracic spine. In Posterior Anterior obtunded patients in whom the thoracic and lumbar spine cannot be evaluated clinically, the radiographs should be obtained routinely during the secondary survey or on admission to hospital. Unstable fractures of the pelvis are often associated with injuries to the lumbar spine. A significant force is normally required to damage the thoracic, lumbar, and sacral segments of the spinal cord, and the skeletal injury is usually evident on the standard anteroposterior and horizontal beam lateral radiographs. Burst fractures, and fractures affecting the posterior facet joints or Supraspinous Anterior pedicles, are unstable and more easily seen on the lateral ligament column radiograph. Instability requires at least two of the three columns of the spine to be disrupted. In simple wedge fractures, only the anterior column is disrupted and the injury remains stable. The demonstration of detail in the thoracic spine can be extremely difficult, particularly in the upper four vertebrae, and computed tomography (CT) is often required Middle Posterior column column Figure 3. Right: CT scan shows the fracture of L4 more clearly, with severe narrowing of the spinal canal. There is a horizontal fracture of the upper part of the vertebral body extending into the posterior elements. Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. Radiol Clin also be caused by sternal or bilateral rib fractures, as the North Am 1997;35:507–32 anterior splinting effect of these structures will be lost. A particular type of fracture, the Chance fracture, is London: BMJ Publishing Group, 1995 typically found in the upper lumbar vertebrae.