2018, School of the Museum of Fine Arts, Boston, Orknarok's review: "Lamisil generic (Terbinafine) 250 mg. Best Lamisil.".
The free energy drop between NADH and CoQ of approximately 13 to 14 PrPr kcal is able to support movement of four protons buy generic lamisil 250mg on line. However discount lamisil 250mg with visa, the FAD in succinate Cys dehydrogenase (as well as ETF-CoQ oxidoreductase and -glycerophosphate dehy- SS S Fe drogenase) is at roughly the same energy level as CoQ buy lamisil 250mg lowest price, and there is no energy Pr Cys S Fe S released as they transfer electrons to CoQ purchase 250mg lamisil with mastercard. These proteins do not span the membrane and consequently do not have a proton pumping mechanism. COENZYME Q SS S Fe CysCys SS CoQ is the only component of the electron transport chain that is not protein bound. PrPr CysCys The large hydrophobic side chain of 10 isoprenoid units (50 carbons) confers lipid PrPr solubility, and CoQ is able to diffuse through the lipids of the inner mitochondrial membrane (Fig. When the oxidized quinone form accepts a single electron, Fig. In Fe-S centers, the Fe 4 4 it forms a free radical (a compound with a single electron in an orbital). The trans- is chelated to free sulfur (S) atoms, and to cys- fer of single electrons makes it the major site for generation of toxic oxygen free teine sulfhydryl groups on proteins. The protein subunits are sometimes called non-heme iron proteins. When these proteins are treated with acid, the The long side chain of CoQ has 10 of the 5-carbon isoprenoid units, and is free sulfur produces hydrogen sulfide (H2S)— sometimes called CoQ10. It is also called ubiquinone (the quinone found every- the familiar smell of rotten eggs. CoQ can be synthesized in the human from precursors derived from carbohy- drates and fat. The long isoprenoid side chain is formed in the pathway that produces the isoprenoid precursors of cholesterol. CoQ10 is sometimes prescribed for patients recovering from a myocardial infarction, in an effort to increase their exercise capacity. O OH OH e– + H+ e– + H+ CH3 3 CH3 CH3O [CH2CH CCH2]10H O •O OH Fully oxidized or Semiquinone form– Reduced or quinol form quinone form (Q) (free radical, Q–•) (dihydroquinol, QH ) 2 Fig. Coenzyme Q contains a quinone with a long lipophilic side chain comprising 10 isoprenoid units (thus, it is sometimes called CoQ10. The mobility of CoQ in the membrane, its ability to accept one or two electrons, and its ability to accept and donate protons enable it to participate in the proton pumps for both complexes I and III as it shuttles electrons between them (see Section I. CYTOCHROMES Although iron deficiency anemia is The remainder of the components in the electron transport chain are cytochromes characterized by decreased levels (see Fig. Each cytochrome is a protein that contains a bound heme (i. Thus, energy is released by electron transfer such as Ann O’Rexia (see Chapter 16), 3 results, in part, from the lack of electron between complexes III and IV. The iron atoms in the cytochromes are in the Fe state. As they accept an electron, they are reduced to Fe2. As they are reoxidized transport for ATP production. COPPER (CU ) AND THE REDUCTION OF OXYGEN The last cytochrome complex is cytochrome oxidase, which passes electrons from cytochrome c to O2 (see Fig. It contains cytochromes a and a3 and the oxygen binding site. A whole oxygen molecule, O2, must accept four electrons to be reduced to 2 H O. Bound copper (Cu ) ions in the cytochrome 2 oxidase complex facilitate the collection of the four electrons and the reduction of O2. Cytochrome oxidase has a much lower Km for O2 than myoglobin (the heme- containing intracellular oxygen carrier) or hemoglobin (the heme-containing oxygen transporter in the blood). Thus, O2 is “pulled” from the erythrocyte to myoglobin, and from myoglobin to cytochrome oxidase, where it is reduced to H2O. CH3 (CH2 CH C CH2)3 H CH CH2 3 H C The iron in the heme in hemoglo- bin, unlike the iron in the heme of HC CH cytochromes, never changes its O 2 C N CH oxidation state (it is Fe in hemoglobin). If 3 the iron in hemoglobin were to become oxi- H N Fe N 3 –COO CH CH CH CH dized (Fe ), the oxygen-binding capacity of 2 2 N 2 the molecule would be lost.
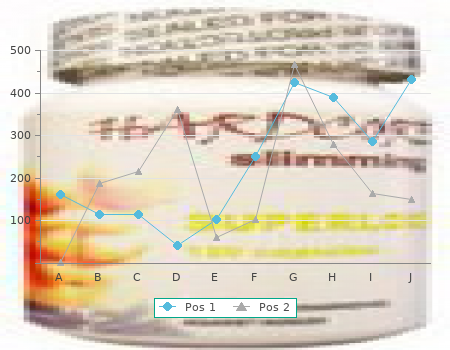
As computer power has increased lamisil 250mg mastercard, there has been a movement to the 13-segment model purchase 250 mg lamisil fast delivery, which includes two feet order lamisil 250 mg without a prescription, two shanks discount lamisil 250 mg overnight delivery, two thighs, two forearms, two upper arms, a pelvis, a trunk, and the head. These cameras are focused on a fixed space in the room, which is as- signed a room coordinate system. All cameras are synchronized to take im- ages at the same time, for gait usually at a rate of 60 frames per second. With current clinical gait analysis systems, this process of identifying the marker and calculating its precise position in three-dimensional space is all auto- mated; however, some error still occurs requiring each patient to be reviewed by a technical person who has experience with the system, usually an indi- vidual trained in biomechanics. Once the marker is identified in space, spe- cialized software defines the specific assigned segment whose motion can then be calculated into clinically defined joint range of motion. The specific joint motion is calculated from the motion of each segment. A problem that occurs in this reduction process is that the motion of the markers includes soft-tissue motion because the markers are not fixed to bones, but are attached to the skin. To counteract soft-tissue movement, the marker path is smoothed to remove high-frequency motion and the segments are assumed to be attached at points that represent accurate anatomic struc- ture, because joints rarely have any measurable motion in translation or dis- traction. These two data manipulations help decrease the soft-tissue artifact; however, soft-tissue motion still has to be considered as a possible measure- ment error in some children if unexplained motion is found. The next major task in the kinematic data reduction is to assign specific clinically recogniz- able joint positions, such as degrees of flexion or rotation. This task requires choosing a method to reduce the three-dimensional data. Understanding this system is important for clinicians because it may explain the size of some of the numbers that do not correlate with physicians’ own assessments. Data Reduction Algorithms All commercially available clinical data reduction software algorithms cur- rently in use reduce the data using Euler angles. This process mimics what clinicians rou- tinely do in physical examinations. For example, when a physician measures a specific contracture of the hip, he would say there is so much abduction, so much flexion, and so much rotation present. The mathematical concepts 278 Cerebral Palsy Management Figure 7. The use of Euler angle calcula- tions is very order dependent; therefore, the order of the calculations has to be understood. For example, the position of the shoulder with a calculation order of 45° internal rota- tion, 45° abduction, and 45° flexion (A) is very different from the position obtained with 45° flexion, 45° abduction, and 45° internal rotation (B). These joints include the hip, shoulder, and subtalar joints. For example, a shoul- der position of 45° flexion, 45° abduction, and 45° internal rotation is very different from 45° internal rotation, 45° abduction, and 45° of flexion (Fig- ure 7. All current kinematic systems have adopted the convention of flex- ion and extension followed by abduction and adduction, then rotation as the order of derotation in the coordinate systems. Based on personal experience, most clinicians seem to rotate out rotation first, or, alternatively, they rotate out the largest plane of motion first. There has been no evaluation of what order clinicians cognitively use for visual or physical examinations; however, the difference is sometimes large enough to make clinicians uncomfortable with the kinematic numbers. There are no right or wrong numbers, as these only reflect the measurement algorithm, and clinicians need to understand that their impression suffers the same faults. Although the Euler angle transformations are currently in primary clinical use, other coordinate transformation systems are used for research and may gradually find a role in clinical practice. The Grood–Suntay technique29 sets up a global coordinate system in each segment with defined positions of the adjacent coordinate system. The easiest but oversimplified explanation of this system is that it functions similar to the assignment of latitude and lon- gitude in the global surface position assignment systems. The advantage of this system is that it is independent of the order of rotation and may better reflect how clinicians look at children; however, we do not think it reflects how clinicians mentally, or by physical examination, assign degrees of de- formity. Another system that is independent of the order of rotation is the finite helical screw approach in which the motion of the mobile coordinate 7.
The Practical Management of Spas- ticity in Children and Adults lamisil 250mg sale. Intrathecal baclofen infusion and sub- sequent orthopedic surgery in patients with cerebral palsy cheap 250mg lamisil. Effect on ambulation of continuous in- trathecal baclofen infusion generic 250mg lamisil overnight delivery. Midthoracic catheter placement for intrathecal baclofen administration in children with quadriplegic spasticity order lamisil 250 mg otc. The effects of magnetic resonance imaging (MRI) on Med- tronic drug infusion systems. Intrathecal baclofen for treatment of spasticity in children. Lioresal in the treatment of neurogenic bladder dys- function. Kofler M, Kronenberg MF, Rifici C, Saltuari L, Bauer G. Epileptic seizures as- sociated with intrathecal baclofen application. Pharmacotherapy of spasticity: Oral medications and intrathecal ba- clofen. Intrathecal drug administration, present use and future trends. The distribution of medication along the spinal cord after chronic intrathecal administration. Meythaler JM, Guin-Renfroe S, Law C, Grabb P, Hadley MN. Continuously in- fused intrathecal baclofen over 12 months for spastic hypertonia in adolescents and adults with cerebral palsy. Long-term continuously infused intrathecal baclofen for spastic-dystonic hypertonia in traumatic brain injury: 1-year experience. Pharmacokinetics of intrathecal baclofen in spas- ticity. Physostigmine in the treatment of intrathecal ba- clofen overdose. Effect of intrathecal baclofen on bladder and sphincter control. Clinical use of polysynap- tic flexion reflexes in the management of spasticity with intrathecal baclofen. Functional outcomes following selective posterior rhizo- tomy in children with cerebral palsy. Intrathecal baclofen for severe spinal spas- ticity. Intrathecal baclofen alleviates spinal cord spasticity. Are baclofen-sensitive GABAb receptors present on primary afferent terminals of the spinal cord? Patient management of cerebral origin spasticity with intrathecal ba- clofen. Indium-111 DTPA flow study to evaluate surgically implanted drug pump delivery system. Baclofen withdrawal presenting as multi-organ system failure. Intrathecal baclofen therapy for treat- ing severe spasticity in pediatric patient with anoxic brain injury. SECTION III Surgical Techniques 1 Upper Extremity Procedures 1. Shoulder Adductor, Extension, and External Rotator Lengthening Indication The indications for shoulder adductor lengthening are usually in a child with a quadriplegic pattern involvement who has a severe shoulder adduction con- tracture making axillary care and dressing difficult. The primary contracture is usually with internal rotation and adduction coming from the pectoralis.