2018, American Bible College and Seminary, Giores's review: "Buspirone 10 mg, 5 mg. Discount Buspirone online in USA.".
Psychotherapy - The discipline of psychotherapy uses ADHD cognitive therapy techniques in addition to other therapeutic strategies order buspirone 10mg with amex. Many children with ADD have co-morbid mental disorders discount 10mg buspirone with visa, such as anxiety and depression buspirone 5 mg with visa. The psychotherapist can discuss issues that bother the child and explore negative behaviors generic buspirone 5mg without a prescription, as well as provide ways to reduce the effects of ADD symptoms. Support Groups and Skills Training ??? Parents and children can attend ADD support group meetings, which include skills training and education about ADHD therapy for children. The meetings provide a support network of other families coping with the disorder. Together, they can discuss common issues and experiences with using the various coping skills and strategies. ADHD therapy techniques address a variety of issues associated with ADHD in children. Common issues dealt with during therapy sessions include:destructive thought patternsdifficulties maintaining friendships and other social relationshipsimpatience and impulsivenessFinding a skilled mental health professional with years of experience providing ADHD therapy for children is very important. Another referral source is your county psychological association. Parents can also search through several ADHD practitioner referral sites on the Internet. Physicians and therapists listing on these services do so because they have experience providing ADHD therapy and likely specialize in it. Natural remedies for ADHD may seem like a viable alternative to taking stimulant-based ADHD medications day after day. Many online ads and late-night television commercials tout a natural cure for ADHD. While tempting to try, most of these natural remedies for ADHD probably will not effectively control the symptoms of ADD. Leading experts and ADHD researchers know of no natural cure for ADHD. Talk to your health care practitioner (see Getting ADHD Help ) before trying any of these natural remedies. Read information and research any claims about remedies you might find interesting from a variety of sources. Numerous special diets and food-avoidance lists, advertised as alternative treatments for ADHD, have gained popularity over the years. One such diet that gained rapid popularity, called the Feingold Diet, involved the methodical elimination of certain food additives and preservatives. Ben Feingold, MD, theorized that these additives and artificial flavorings caused hyperactivity in children; thus, their elimination would reduce hyperactive behavior. Others proponents of dietary manipulations as alternative treatments for ADHD postulated that dietary sugar and simple carbohydrates could cause ADHD in children. This sugar elimination diet has caused a significant amount of controversy over the years. Although research shows that ingesting refined sugars and carbohydrates can cause an activity spike for the child, due to a rapid increase in blood glucose, the heightened activity lasts a short period of time and a period of decreased activity often follows. Likewise, taking zinc supplements, as a natural ADD treatment has no measurable effect on children diagnosed with the disorder. Furthermore, long-term use of zinc can cause anemia in those without a zinc deficiency. Omega-3 fatty acids, called essential fatty acids, provide an important piece of the components necessary for normal brain function. The omega-3 fatty acids, found naturally in certain fish and vegetable oils, may benefit people with ADHD, but more research is needed. Experts do not know whether supplementary docosahexaenoic acid (DHA) or eicosapentaneoic acid (EPA) offers any benefits as a natural ADD treatment. One alternative approach for treatment of ADHD without medication uses daily massage therapy.
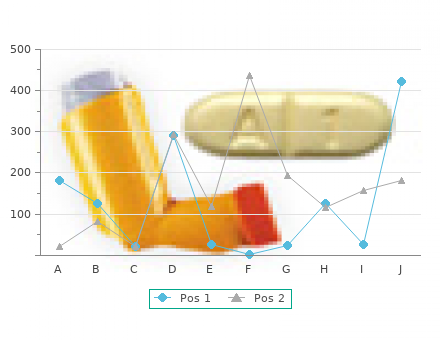
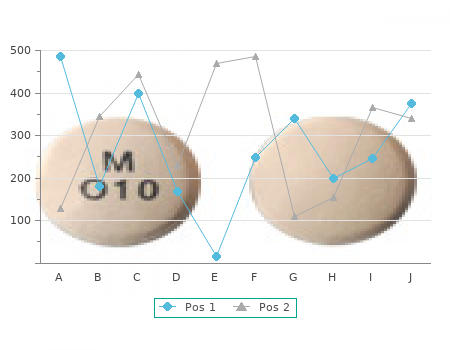
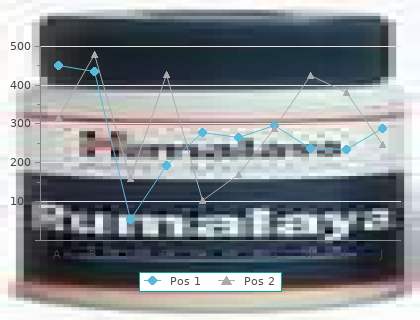
The patients recruited as participants in each study had mean scores on ADAS-cog of approximately 23 units order buspirone 10mg fast delivery, with a range from 1 to 61 generic buspirone 10 mg amex. Lesser degrees of change discount buspirone 10 mg fast delivery, however 5 mg buspirone mastercard, are seen in patients with very mild or very advanced disease because the ADAS-cog is not uniformly sensitive to change over the course of the disease. The annualized rate of decline in the placebo patients participating in Exelon trials was approximately 3-8 units per year. The CIBIC-Plus is not a single instrument and is not a standardized instrument like the ADAS-cog. Clinical trials for investigational drugs have used a variety of CIBIC formats, each different in terms of depth and structure. As such, results from a CIBIC-Plus reflect clinical experience from the trial or trials in which it was used and can not be compared directly with the results of CIBIC-Plus evaluations from other clinical trials. The CIBIC-Plus used in the Exelon trials was a structured instrument based on a comprehensive evaluation at baseline and subsequent time-points of three domains: patient cognition, behavior and functioning, including assessment of activities of daily living. It represents the assessment of a skilled clinician using validated scales based on his/her observation at interviews conducted separately with the patient and the caregiver familiar with the behavior of the patient over the interval rated. The CIBIC-Plus is scored as a seven point categorical rating, ranging from a score of 1, indicating "markedly improved," to a score of 4, indicating "no change" to a score of 7, indicating "marked worsening. In a study of 26 weeks duration, 699 patients were randomized to either a dose range of 1-4 mg or 6-12 mg of Exelon per day or to placebo, each given in divided doses. The 26-week study was divided into a 12-week forced dose titration phase and a 14-week maintenance phase. The patients in the active treatment arms of the study were maintained at their highest tolerated dose within the respective range. Effects on the ADAS-cog: Figure 1 illustrates the time course for the change from baseline in ADAS-cog scores for all three dose groups over the 26 weeks of the study. At 26 weeks of treatment, the mean differences in the ADAS-cog change scores for the Exelon-treated patients compared to the patients on placebo were 1. Both treatments were statistically significantly superior to placebo and the 6-12 mg/day range was significantly superior to the 1-4 mg/day range. Figure 2 illustrates the cumulative percentages of patients from each of the three treatment groups who had attained at least the measure of improvement in ADAS-cog score shown on the X axis. Three change scores, (7-point and 4-point reductions from baseline or no change in score) have been identified for illustrative purposes, and the percent of patients in each group achieving that result is shown in the inset table. The curves demonstrate that both patients assigned to Exelon and placebo have a wide range of responses, but that the Exelon groups are more likely to show the greater improvements. A curve for an effective treatment would be shifted to the left of the curve for placebo, while an ineffective or deleterious treatment would be superimposed upon, or shifted to the right of the curve for placebo, respectively. Effects on the CIBIC-Plus: Figure 3 is a histogram of the frequency distribution of CIBIC-Plus scores attained by patients assigned to each of the three treatment groups who completed 26 weeks of treatment. The mean Exelon-placebo differences for these groups of patients in the mean rating of change from baseline were 0. The mean ratings for the 6-12 mg/day and 1-4 mg/day groups were statistically significantly superior to placebo. The differences between the 6-12 mg/day and the 1-4 mg/day groups were statistically significant. In a second study of 26 weeks duration, 725 patients were randomized to either a dose range of 1-4 mg or 6-12 mg of Exelon per day or to placebo, each given in divided doses. The 26-week study was divided into a 12-week forced dose titration phase and a 14-week maintenance phase. The patients in the active treatment arms of the study were maintained at their highest tolerated dose within the respective range. Effects on the ADAS-cog: Figure 4 illustrates the time course for the change from baseline in ADAS-cog scores for all three dose groups over the 26 weeks of the study. At 26 weeks of treatment, the mean differences in the ADAS-cog change scores for the Exelon-treated patients compared to the patients on placebo were 0. The 6-12 mg/day group was statistically significantly superior to placebo, as well as to the 1-4 mg/day group. The difference between the 1-4 mg/day group and placebo was not statistically significant. Figure 5 illustrates the cumulative percentages of patients from each of the three treatment groups who had attained at least the measure of improvement in ADAS-cog score shown on the X axis.
Dose adjustment of OC dose is not required when coadministered with Latuda safe buspirone 10mg. There are no adequate and well-controlled studies of Latuda in pregnant women purchase buspirone 10mg line. No teratogenic effects were seen in studies in which pregnant rats and rabbits were given lurasidone during the period of organogenesis at doses up to 25 and 50 mg/kg/day order buspirone 5 mg overnight delivery, respectively purchase buspirone 10mg on-line. These doses are 3 and 12 times, in rats and rabbits respectively, the maximum recommended human dose (MRHD) of 80 mg/day based on body surface area. No adverse developmental effects were seen in a study in which pregnant rats were given lurasidone during the period of organogenesis and continuing through weaning at doses up to 10 mg/kg/day; this dose is approximately equal to the MRHD based on body surface area. Non-teratogenic EffectsNeonates exposed to antipsychotic drugs during the third trimester of pregnancy are at risk for extrapyramidal and/or withdrawal symptoms following delivery. There have been reports of agitation, hypertonia, hypotonia, tremor, somnolence, respiratory distress and feeding disorder in these neonates. These complications have varied in severity; while in some cases symptoms have been self-limited, in other cases neonates have required intensive care unit support and prolonged hospitalization. Latuda should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. The effect of Latuda on labor and delivery in humans is unknown. Latuda was excreted in milk of rats during lactation. It is not known whether Latuda or its metabolites are excreted in human milk. Breast feeding in women receiving Latuda should be considered only if the potential benefit justifies the potential risk to the child. Safety and effectiveness in pediatric patients have not been established. Clinical studies of Latuda in the treatment of schizophrenia did not include sufficient numbers of patients aged 65 and older to determine whether or not they respond differently from younger patients. In elderly patients with psychosis (65 to 85), lurasidone concentrations (20 mg/day) were similar to those in young subjects [see Clinical Pharmacology ]. No dose adjustment is necessary in elderly patients. Elderly patients with dementia-related psychosis treated with Latuda are at an increased risk of death compared to placebo. Latuda is not approved for the treatment of patients with dementia-related psychosis [see Boxed Warning ]. It is recommended that Latuda dose should not exceed 40 mg/day in patients with moderate and severe renal impairment (Clcr ?-U 10 mL/min to < 50 mL/min). After administration of a single dose of 40 mg Latuda to patients with mild, moderate and severe renal impairment, mean Cmax increased by 40%, 92% and 54%, respectively and mean AUC(0-b) increased by 53%, 91% and 2- times, respectively compared to healthy matched subjects. It is recommended that Latuda dose should not exceed 40 mg/day in patients with moderate and severe hepatic impairment (Child-Pugh Class B and C). In a single-dose study of Latuda 20 mg, lurasidone mean AUC(0-last) was 1. Population pharmacokinetic evaluation indicated that the mean AUC of Latuda was 18% higher in women than in men, and correspondingly, the apparent oral clearance of Latuda was lower in women. Mean Cmax of Latuda was similar between women and men. No dosage adjustment of Latuda is recommended based on gender. Although no specific pharmacokinetic study was conducted to investigate the effects of race on the disposition of Latuda, population pharmacokinetic evaluation revealed no evidence of clinically significant race-related differences in the pharmacokinetics of Latuda. No dosage adjustment of Latuda is recommended based on race. Based on in vitro studies utilizing human liver enzymes, Latuda is not a substrate for CYP1A2; smoking is therefore not expected to have an effect on the pharmacokinetics of Latuda. Latuda has not been systematically studied in humans for its potential for abuse or physical dependence or its ability to induce tolerance. While clinical studies with Latuda did not reveal any tendency for drug-seeking behavior, these observations were not systematic and it is not possible to predict the extent to which a CNS-active drug will be misused, diverted and/or abused once it is marketed.
Buspirone (Buspar generic) 10mg, 5mg